1396/09/15 21:12:49

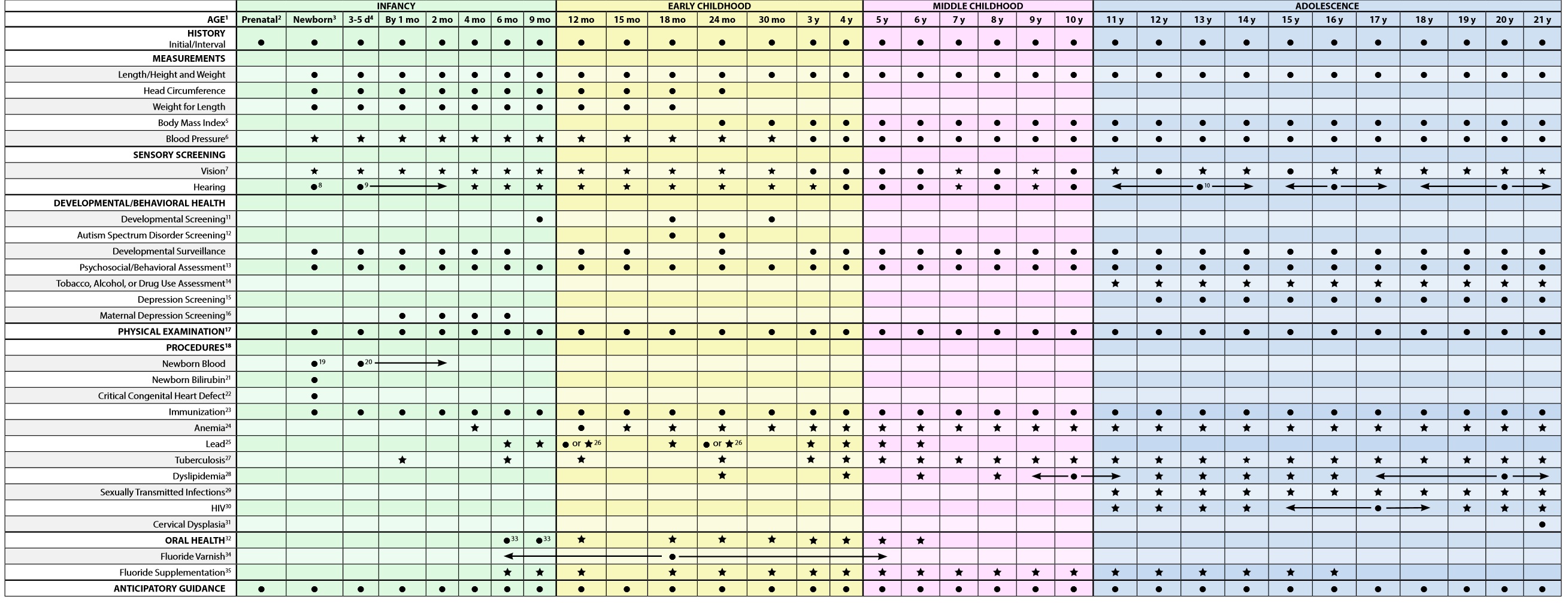
پزشکان کودکان همواره مورد این سوال قرار می گیرند که در چه سنی کودکم را مورد بررسی شنوایی ،بینایی و ارزیابی تکاملی وارزیابی ازمایشگاهی قرار دهم .جدول ذیل و توضیحات ان که به تدریج انرا به زبان فارسی برخواهم گرداند به این سوالات بر طبق استانداردهای نوین طب کودکان پاسخ می دهد .
هر کودک و خانواده منحصر بفرد است و با دیگر کودکان و خانواده ها متفاوت است .این توصیه های پیشگیری در مراقبت کودکان، برای کودکانی طراحی شده که مراقبت والدین کافی و در خور دارند و تظاهری از بیماری های مهم ندارند و رشد و تکامل رضایت بخشی دارند.
.کودکان و نوجوانانی که مسایل عمده ای در زمینه تکاملی ،روانی اجتماعی ،و بیماری های مزمن دارند ممکن است نیازمند مشاوره و ویزیت های درمانی مکرر علاوه بر ویزیت های مراقبت پیشگیری باشند .ویزیت های اضافه ممکن است در موارد وجود شرایط طبیعی ولی متفاوت با دیگر کودکان لازم باشد .
1. If a child comes under care for the first time at any point on the schedule, or if any items are not accomplished at the suggested age, the schedule should be brought up-to-date at the earliest possible time.
1-در صورتی که کودک برای بار اول در هر کجای برنامه تحت مراقبت قرار گیرد یا در صورتی که هر مورد در سن توصیه شده انجام نشده باشد .در سریعترین زمان ممکن باید کودک را به برنامه رساند.
2. A prenatal visit is recommended for parents who are at high risk, for first-time parents, and for those who request a conference. The prenatal visit should include anticipatory guidance, pertinent medical history, and a discussion of benefits of breastfeeding and planned method of feeding, per “The Prenatal Visit” (http://pediatrics.aappublications.org/ content/124/4/1227.full).
2-ویزیت قبل از تولد برای والدین پرخطر و والدینی که برای اولین بار صاحب فرزند میشوند و درخواست مشاوره دارند توصیه می شود .در این ویزیت مخاطرات پیش رو و اقدامات لازم گوشزد شده ،شرح حال پزشکی اخذ می گردد و در خصوص منافع تغذیه با شیر مادر و سایر روش های تغذیه اموزش داده می شود .
3. Newborns should have an evaluation after birth, and breastfeeding should be encouraged (and instruction and support should be offered).
3-نوزادان پس از تولد باید ویزیت شده و تغذیه با شیر مادر مورد تشویق قرار گیرد و دستورالعمل به اموزش داده شده و حمایت کافی از وی به عمل می اید .
4-نوزادان 3الی 5روز پس از تولد و 48الی 72ساعت پس از ترخیص از بیمارستان مورد ارزیابی مجدد قرار می گیرند و در این ویزیت وضعیت زردی و تغذیه نوزاد ارزیابی می گردد .
5. Screen, per “Expert Committee Recommendations Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity: Summary Report” (http://pediatrics.aappublications.org/content/120/ Supplement_4/S164.full).
5-غربالگری از نظر اضافه وزن و چاقی ضروری است .
6. Blood pressure measurement in infants and children with specific risk conditions should be performed at visits before age 3 years.
6- اندازه گیری فشار خون در شیرخواران و کودکان با شرایط خطر خاص در ویزیت های قبل از سه سالگی باید انجام شود
7-سنجش بینایی در سن چهار الی پنج سالگی و درکودکان سه ساله که همکاری می کنند توصیه می شود .
7. A visual acuity screen is recommended at ages 4 and 5 years, as well as in cooperative 3-year-olds. Instrument-based screening may be used to assess risk at ages 12 and 24 months, in addition to the well visits at 3 through 5 years of age. See “Visual System Assessment in Infants, Children, and Young Adults by Pediatricians” (http://pediatrics.aappublications. org/content/137/1/e20153596) and “Procedures for the Evaluation of the Visual System by Pediatricians” (http://pediatrics.aappublications.org/content/137/1/e20153597).
غربالگری با وسایل تشخیصی ممکن است برای تعیین میزان خطر درگیری در 12تا 24 ماهگی علاوه بر ویزیت های سه تا پنج سالگی استفاده شود .
8. Confirm initial screen was completed, verify results, and follow up, as appropriate. Newborns should be screened, per “Year 2007 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs” (http://pediatrics.aappublications.org/content/120/4/898.full).
8-از انجام شدن کامل غربالگری اولیه مطمئن شوید .نتایج را بررسی کنید و پیگیری متناسب را برنامه ریزی کنید .
9. Verify results as soon as possible, and follow up, as appropriate.
9-نتایج را به سرعت بررسی کنید و پیگیری متناسب را برنامه ریزی کنید
10. Screen with audiometry including 6,000 and 8,000 Hz high frequencies once between 11 and 14 years, once between 15 and 17 years, and once between 18 and 21 years. See “The Sensitivity of Adolescent Hearing Screens Significantly Improves by Adding High Frequencies” (http://www.jahonline.org/article/S1054-139X(16)00048-3/fulltext).
10-بین 11 تا 14سالگی با فرکانس بالای 6000-80000 و بین 15تا 17سالگی یک بار و بین 18تا 21سالگی یک بار ادیومتری غربالگری انجام دهید .
11. See “Identifying Infants and Young Children With Developmental Disorders in the Medical Home: An Algorithm for Developmental Surveillance and Screening” (http://pediatrics.aappublications.org/content/118/1/405.full).
12. Screening should occur per “Identification and Evaluation of Children With Autism Spectrum Disorders” (http://pediatrics.aappublications.org/content/120/5/1183.full).
13. This assessment should be family centered and may include an assessment of child social-emotional health, caregiver depression, and social determinants of health. See “Promoting Optimal Development: Screening for Behavioral and Emotional Problems” (http://pediatrics.aappublications.org/content/135/2/384) and “Poverty and Child Health in the United States” (http://pediatrics.aappublications.org/content/137/4/e20160339).
14. A recommended assessment tool is available at http://www.ceasar-boston.org/CRAFFT/index.php.
15. Recommended screening using the Patient Health Questionnaire (PHQ)-2 or other tools available in the GLAD-PC toolkit and at http://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/Mental-Health/Documents/MH_ ScreeningChart.pdf. ) 16. Screening should occur per “Incorporating Recognition and Management of Perinatal and Postpartum Depression Into Pediatric Practice” (http://pediatrics.aappublications.org/content/126/5/1032).
17. At each visit, age-appropriate physical examination is essential, with infant totally unclothed and older children undressed and suitably draped. See “Use of Chaperones During the Physical Examination of the Pediatric Patient” (http://pediatrics.aappublications.org/content/127/5/991.full).
18. These may be modified, depending on entry point into schedule and individual need. (continued)
19. Confirm initial screen was accomplished, verify results, and follow up, as appropriate. The Recommended Uniform Newborn Screening Panel (http://www.hrsa.gov/ advisorycommittees/mchbadvisory/heritabledisorders/recommendedpanel/ uniformscreeningpanel.pdf), as determined by The Secretary’s Advisory Committee on Heritable Disorders in Newborns and Children, and state newborn screening laws/regulations (http://genes-r-us.uthscsa.edu/sites/genes-r-us/files/ nbsdisorders.pdf) establish the criteria for and coverage of newborn screening procedures and programs.
20. Verify results as soon as possible, and follow up, as appropriate.
21. Confirm initial screening was accomplished, verify results, and follow up, as appropriate. See “Hyperbilirubinemia in the Newborn Infant ≥35 Weeks’ Gestation: An Update With Clarifications” (http://pediatrics.aappublications.org/ content/124/4/1193).
22. Screening for critical congenital heart disease using pulse oximetry should be performed in newborns, after 24 hours of age, before discharge from the hospital, per “Endorsement of Health and Human Services Recommendation for Pulse Oximetry Screening for Critical Congenital Heart Disease” (http://pediatrics. aappublications.org/content/129/1/190.full).
23. Schedules, per the AAP Committee on Infectious Diseases, are available at http://redbook.solutions.aap.org/SS/Immunization_Schedules.aspx. Every visit should be an opportunity to update and complete a child’s immunizations.
24. See “Diagnosis and Prevention of Iron Deficiency and Iron-Deficiency Anemia in Infants and Young Children (0–3 Years of Age)” (http://pediatrics.aappublications. org/content/126/5/1040.full).
25. For children at risk of lead exposure, see “Low Level Lead Exposure Harms Children: A Renewed Call for Primary Prevention” (http://www.cdc.gov/nceh/lead/ACCLPP/ Final_Document_030712.pdf).
26. Perform risk assessments or screenings as appropriate, based on universal screening requirements for patients with Medicaid or in high prevalence areas.
27. Tuberculosis testing per recommendations of the AAP Committee on Infectious Diseases, published in the current edition of the AAP Red Book: Report of the Committee on Infectious Diseases. Testing should be performed on recognition of high-risk factors.
28. See “Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents” (http://www.nhlbi.nih.gov/guidelines/cvd_ped/index.htm).
29. Adolescents should be screened for sexually transmitted infections (STIs) per recommendations in the current edition of the AAP Red Book: Report of the Committee on Infectious Diseases.
30. Adolescents should be screened for HIV according to the USPSTF recommendations (http://www.uspreventiveservicestaskforce.org/uspstf/uspshivi.htm) once between the ages of 15 and 18, making every effort to preserve confidentiality of the adolescent. Those at increased risk of HIV infection, including those who are sexually active, participate in injection drug use, or are being tested for other STIs, should be tested for HIV and reassessed annually.
31. See USPSTF recommendations (http://www.uspreventiveservicestaskforce.org/ uspstf/uspscerv.htm). Indications for pelvic examinations prior to age 21 are noted in “Gynecologic Examination for Adolescents in the Pediatric Office Setting” (http://pediatrics.aappublications.org/content/126/3/583.full).
32. Assess whether the child has a dental home. If no dental home is identified, perform a risk assessment (http://www2.aap.org/oralhealth/docs/RiskAssessmentTool.pdf) and refer to a dental home. Recommend brushing with fluoride toothpaste in the proper dosage for age. See “Maintaining and Improving the Oral Health of Young Children” (http://pediatrics.aappublications.org/content/134/6/1224).
33. Perform a risk assessment (http://www2.aap.org/oralhealth/docs/ RiskAssessmentTool.pdf). See “Maintaining and Improving the Oral Health of Young Children” (http://pediatrics.aappublications.org/content/134/6/1224).
34. See USPSTF recommendations (http://www.uspreventiveservicestaskforce.org/ uspstf/uspsdnch.htm). Once teeth are present, fluoride varnish may be applied to all children every 3–6 months in the primary care or dental office. Indications for fluoride use are noted in “Fluoride Use in Caries Prevention in the Primary Care Setting” (http://pediatrics.aappublications.org/content/134/3/626).
35. If primary water source is deficient in fluoride, consider oral fluoride supplementation. See “Fluoride Use in Caries Prevention in the Primary Care Setting” (http://pediatrics. aappublications.org/content/134/3/626).
Summary of Changes Made to the Bright Futures/AAP Recommendations for Preventive Pediatric Health Care (Periodicity Schedule)
This schedule reflects changes approved in February 2017 and published in April 2017. For updates, visit www.aap.org/periodicityschedule. For further information, see the Bright Futures Guidelines, 4th Edition, Evidence and Rationale chapter (https://brightfutures.aap.org/Bright%20Futures%20Documents/BF4_Evidence_Rationale.pdf).
CHANGES MADE IN FEBRUARY 2017
HEARING • Timing and follow-up of the screening recommendations for hearing during the infancy visits have been delineated. Adolescent risk assessment has changed to screening once during each time period.
• Footnote 8 has been updated to read as follows: “Confirm initial screen was completed, verify results, and follow up, as appropriate. Newborns should be screened, per ‘Year 2007 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs’ (http://pediatrics.aappublications.org/content/120/4/898.full).”
• Footnote 9 has been added to read as follows: “Verify results as soon as possible, and follow up, as appropriate.”
• Footnote 10 has been added to read as follows: “Screen with audiometry including 6,000 and 8,000 Hz high frequencies once between 11 and 14 years, once between 15 and 17 years, and once between 18 and 21 years. See ‘The Sensitivity of Adolescent Hearing Screens Significantly Improves by Adding High Frequencies’ (http://www.jahonline.org/article/S1054-139X(16)00048-3/fulltext).”
PSYCHOSOCIAL/BEHAVIORAL ASSESSMENT
• Footnote 13 has been added to read as follows: “This assessment should be family centered and may include an assessment of child social-emotional health, caregiver depression, and social determinants of health. See ‘Promoting Optimal Development: Screening for Behavioral and Emotional Problems’ (http://pediatrics.aappublications.org/content/135/2/384) and ‘Poverty and Child Health in the United States’ (http://pediatrics.aappublications.org/content/137/4/e20160339).”
TOBACCO, ALCOHOL, OR DRUG USE ASSESSMENT
• The header was updated to be consistent with recommendations.
DEPRESSION SCREENING • Adolescent depression screening begins routinely at 12 years of age (to be consistent with recommendations of the US Preventive Services Task Force [USPSTF]).
MATERNAL DEPRESSION SCREENING • Screening for maternal depression at 1-, 2-, 4-, and 6-month visits has been added.
• Footnote 16 was added to read as follows: “Screening should occur per ‘Incorporating Recognition and Management of Perinatal and Postpartum Depression Into Pediatric Practice’ (http://pediatrics.aappublications.org/content/126/5/1032).”
NEWBORN BLOOD • Timing and follow-up of the newborn blood screening recommendations have been delineated.
• Footnote 19 has been updated to read as follows: “Confirm initial screen was accomplished, verify results, and follow up, as appropriate. The Recommended Uniform Newborn Screening Panel (http://www.hrsa.gov/advisorycommittees/mchbadvisory/ heritabledisorders/recommendedpanel/uniformscreeningpanel.pdf), as determined by The Secretary’s Advisory Committee on Heritable Disorders in Newborns and Children, and state newborn screening laws/regulations (http://genes-r-us.uthscsa.edu/sites/ genes-r-us/files/nbsdisorders.pdf) establish the criteria for and coverage of newborn screening procedures and programs.”
• Footnote 20 has been added to read as follows: “Verify results as soon as possible, and follow up, as appropriate.”
NEWBORN BILIRUBIN • Screening for bilirubin concentration at the newborn visit has been added.
• Footnote 21 has been added to read as follows: “Confirm initial screening was accomplished, verify results, and follow up, as appropriate. See ‘Hyperbilirubinemia in the Newborn Infant ≥35 Weeks’ Gestation: An Update With Clarifications’ (http://pediatrics.aappublications.org/content/124/4/1193).”
DYSLIPIDEMIA
• Screening for dyslipidemia has been updated to occur once between 9 and 11 years of age, and once between 17 and 21 years of age (to be consistent with guidelines of the National Heart, Lung, and Blood Institute).
SEXUALLY TRANSMITTED INFECTIONS
• Footnote 29 has been updated to read as follows: “Adolescents should be screened for sexually transmitted infections (STIs) per recommendations in the current edition of the AAP Red Book: Report of the Committee on Infectious Diseases.”
HIV
• A subheading has been added for the HIV universal recommendation to avoid confusion with STIs selective screening recommendation.
• Screening for HIV has been updated to occur once between 15 and 18 years of age (to be consistent with recommendations of the USPSTF). • Footnote 30 has been added to read as follows: “Adolescents should be screened for HIV according to the USPSTF recommendations (http://www.uspreventiveservicestaskforce.org/uspstf/uspshivi.htm) once between the ages of 15 and 18, making every effort to preserve confidentiality of the adolescent. Those at increased risk of HIV infection, including those who are sexually active, participate in injection drug use, or are being tested for other STIs, should be tested for HIV and reassessed annually.”
ORAL HEALTH
• Assessing for a dental home has been updated to occur at the 12-month and 18-month through 6-year visits. A subheading has been added for fluoride supplementation, with a recommendation from the 6-month through 12-month and 18-month through 16-year visits. • Footnote 32 has been updated to read as follows: “Assess whether the child has a dental home. If no dental home is identified, perform a risk assessment (http://www2.aap.org/oralhealth/docs/RiskAssessmentTool.pdf) and refer to a dental home. Recommend brushing with fluoride toothpaste in the proper dosage for age. See ‘Maintaining and Improving the Oral Health of Young Children’ (http://pediatrics.aappublications.org/content/134/6/1224).”
• Footnote 33 has been updated to read as follows: “Perform a risk assessment (http://www2.aap.org/oralhealth/docs/ RiskAssessmentTool.pdf). See ‘Maintaining and Improving the Oral Health of Young Children’ (http://pediatrics.aappublications.org/ content/134/6/1224).”
• Footnote 35 has been added to read as follows: “If primary water source is deficient in fluoride, consider oral fluoride supplementation. See ‘Fluoride Use in Caries Prevention in the Primary Care Setting’ (http://pediatrics.aappublications.org/ content/134/3/626).”
خلاصه تغییرات 2017
Summary of Changes Made to the 2017 Recommendations
HEARING
- Timing and follow-up of the screening recommendations for hearing during the infancy visits have been delineated.
- The accompanying footnotes (#8 & #9) has been updated and added.
- Adolescent hearing risk assessment has changed to screening once during each time period
- An accompanying footnote (#10) has been added.
- An accompanying footnote (#10) has been added.
PSYCHOSOCIAL/BEHAVIORAL ASSESSMENT
- An accompanying footnote (#13) has been added.
TOBACCO, ALCOHOL, OR DRUG USE ASSESSMENT
- The header was updated to be consistent with recommendations.
DEPRESSION SCREENING
- Adolescent depression screening begins routinely at 12 years of age.
MATERNAL DEPRESSION SCREENING
- Screening for maternal depression at 1-, 2-, 4-, and 6-month visits has been added.
- An accompanying footnote (#16) has been added.
NEWBORN BLOOD
- Timing and follow-up of the newborn blood screening recommendations have been delineated.
- The accompanying footnotes (#19 & #20) has been updated and added.
NEWBORN BILIRUBIN
- Screening for bilirubin concentration at the newborn visit has been added.
- An accompanying footnote (#21) has been added.
DYSLIPIDEMIA
- Screening for dyslipidemia has been updated to occur once between 9 and 11 years of age, and once between 17 and 21 years of age.
SEXUALLY TRANSMITTED INFECTIONS (STIs)
- An accompanying footnote (#29) has been added.
HIV
- Screening for HIV has been updated to occur once between 15 and 18 years of age.
- A subheading has been added for the HIV universal recommendation to avoid confusion with STIs selective screening recommendation.
- An accompanying footnote (#30) has been added.
ORAL HEALTH
- Assessing for a dental home has been updated to occur at the 12-month and 18-month through 6-year visits.
- The accompanying footnotes (#32 & #33) have been updated.
- A subheading has been added for fluoride supplementation, with a recommendation from the 6-month through 12-month and 18-month through 16-year visits.
- An accompanying footnote (#35) has been added.